An intracranial hemorrhage, also known as a brain bleed, is a medical emergency that is time sensitive and requires immediate medical attention. This type of bleeding occurs when an artery or blood vessel is ruptured and leaks blood within brain tissue or the meninges (within the skull). The subarachnoid hemorrhage (SAH) is a life-threatening stroke caused by the bleeding within in the subarachnoid space between the arachnoid and pia membranes.
The Cause
The two main causes of a SAH include a recent head trauma or an aneurysm. MayoClinic describes an aneurysm as a blood clot in the brain that looks like a “berry on a stem”. When this “berry” bursts, it causes the blood to stream into the subarachnoid space. The build up of blood is dangerous because it can apply pressure on the brain tissue and restrict oxygen flow. Unfortunately, aneurysms are often undetected and can spontaneously rupture. Studies show that majority of patients who suffer from aneurysms are above 40 years of age, however it is not uncommon for patients younger than 40 years of age to have an aneurysm. When there is a head injury (fall or direct hit) the force of the trauma can cause a blood vessel or artery to tear and seep blood into the subarachnoid space. A brain bleed can be prevented status post a head injury if the patient undergoes imaging to rule out the risks. Some other causes of a subarachnoid hemorrhage include hypertension, atherosclerosis, cocaine use, smoking, family history of aneurysms, sickle cell anemia, cerebral amyloid angiopathy, and anticoagulation disorders.

Pathophysiology
Most SAH are caused by a saccular aneurysm that is a thin extension of an intracranial artery. Typically, these intracranial arteries will have very thin tunica medias and absent elastic lamina making it easier for the artery to break and leak out blood. Increase in heart rate and blood pressure over a prolonged period of time can wear out the walls of arteries and lead to weakening function and aneurysm development. Even the healthiest people can suffer from aneurysms. If the bleeding is not stopped, it can continue to build pressure within the meninges and brain tissue until brain cells begin dying due to oxygen deprivation. It takes about 3-4 minutes of oxygen deprivation to kill brain cells leading to irreversible damage.
History of Present Illness
The patient’s history of current symptoms will be crucial to address SAH and treat it immediately. The tell-tale sign of a brain bleed is a “thunderclap headache” or “the worst headache of your life”. Patients often describe this extremely painful headache as a sudden and sharp headache unlike any other headache they’ve had before. Patients will also present with associated neck stiffness. The neck stiffness indicates meningeal irritation. Other symptoms of SAH are vomiting, confusion, weakness, hemi-paresis, and seizures (more common in patients with ruptured aneurysms). Increase in intracranial pressure can result in brain herniation presenting as asymmetrical pupils (uneven size of pupils). On the physical exam, physicians will look out for motor function and oculomotor function and palsy (indicates a posterior artery as the supplier of blood). In particular, they look for the Kernig sign in which the patient is unable to extend their knee when is at a 90 degree angle and flexed at the thigh. They also check for a positive Brudinski sign indicative of SAH when the patient is unable to extend their hip or knees with passive neck movement. If these tests are positive, the physician will obtain either a head CT scan or MRI to rule out a SAH. The earlier the SAH is diagnosed and treated, the better prognosis of the patient. Many patients will enter the ER with a brain bleed, but stay for further treatment of cardiac arrhythmias or cardiac arrest. Even worse, some patients come into the ER too late and do not make it.

Assessment
If the patient’s symptoms are within a 6 hour window, a non-contrast head CT scan will be able detect the bleeding. In the cases where the CT results are negative that contradicts the patient’s history and symptoms, the physician can do a lumbar puncture to obtain cerebrospinal fluid. The elevated red blood cell count and bilirubin (metabolizes within 12 hours) can indicate a SAH. Studies have shown that 3% of cases with negative head CT scans were positive on the lumbar puncture. For symptoms that have a longer window, an MRI will be more sensitive compared to a head CT. The CTA scan (CT angiography) can detect the type of aneurysmal bleed.

Treatment
The next step the physician will take is deciding the treatment method. Patients with early neurological deterioration or progressive ventricular enlargement can have the cerebrospinal fluid or blood removed through an external ventricular drain. Draining the excess blood or fluid will release the intracranial pressure before brain cells are damaged. Surgical removal of blood will be necessary for patients with large hematomas, focal neuro deficits, or declining level of consciousness. There are 2 different options when neurosurgery is considered.
An aneurysm located on the middle cerebral artery will require clipping via crainotomy. The ruptured artery can be viewed through the crainotomy and clipped at the area that is leaking. This can be seen at figure 4 below.

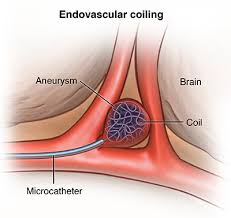
Basilar and posterior cerebral artery aneurysms are treated with coiling in which a catheter is inserted through the femoral artery to coil the area of the bleed as seen in figure 5.
Once these procedures are done, the patient will need close follow ups to prevent bleeding reoccurances. Medications that act as calcium channel blockers are used to prevent vasopasms (narrowing of the arteries due to increased vasoconstriction). Common calcium channel blockers are nicardipine and nimodipine. Vasopasms are concerning because it can result in ischemic brain injury.
A subarachnoid hemorrhage is a devastating type of stroke. While it is not the leading cause of death, it does not have the best prognosis. Look for signs of a brain bleed before it is too late.
References
“Brain Aneurysm.” Mayo Clinic, Mayo Foundation for Medical Education and Research, 9 Aug. 2019, http://www.mayoclinic.org/diseases-conditions/brain-aneurysm/symptoms-causes/syc-20361483.
Kairys, Norah. “Acute Subarachnoid Hemorrhage (SAH).” StatPearls [Internet]., U.S. National Library of Medicine, 10 Aug. 2020, http://www.ncbi.nlm.nih.gov/books/NBK518975/.
Singer, Robert J, et al. “Aneurysmal Subarachnoid Hemorrhage: Epidemiology, Risk Factors, and Pathogenesis.” UpToDate, 1 Nov. 2019, http://www.uptodate.com/contents/aneurysmal-subarachnoid-hemorrhage-epidemiology-risk-factors-and-pathogenesis.
Ziu, Endrit. “Subarachnoid Hemorrhage.” StatPearls [Internet]., U.S. National Library of Medicine, 8 Aug. 2020, http://www.ncbi.nlm.nih.gov/books/NBK441958/.
.
